(866) 755-7519
(866) 755-7519








The Pulse | January 2021
Letter from Leadership

A message to our partners, from CardioSolution President, Perrin Peacock:
I hope you all had a wonderful holiday season and were able to spend quality time with your families as we close out 2020, one of the most challenging years we have ever seen.
As we put this crazy year in the rear view mirror, I wanted to reflect on some of the amazing things we were able to accomplish this year. Together, we:
- Launched the first interventional cardiology program in 5 different communities across 4 states, providing heart care close to home for millions of people.
- Saved more than 1,500 lives.
- Continued to provide emergency heart care for our patients through a global pandemic.
If 2020 taught us anything, it’s that when we join forces, we’re capable of anything. No matter what challenges lie ahead as we continue to navigate these unprecedented times, know that the CardioSolution team is committed to serving you and your patients every day.
Best wishes in the new year,
Perrin Peacock, Co-Founder and President
2021 Billing & Coding Update
Coding Alert
New Changes for Office and Other Outpatient Services Evaluation and Management (E/M) Codes Started on January 1, 2021
The Centers for Medicare and Medicaid (CMS) finalized implementation of major changes to the E/M codes implemented by the AMA CPT Editorial Panel. Changes take effect January 1, 2021. These changes only apply to the office E/M codes and include an increase in values. Some changes include:
- History and exam no longer used to select the level of code for office and other outpatient visits
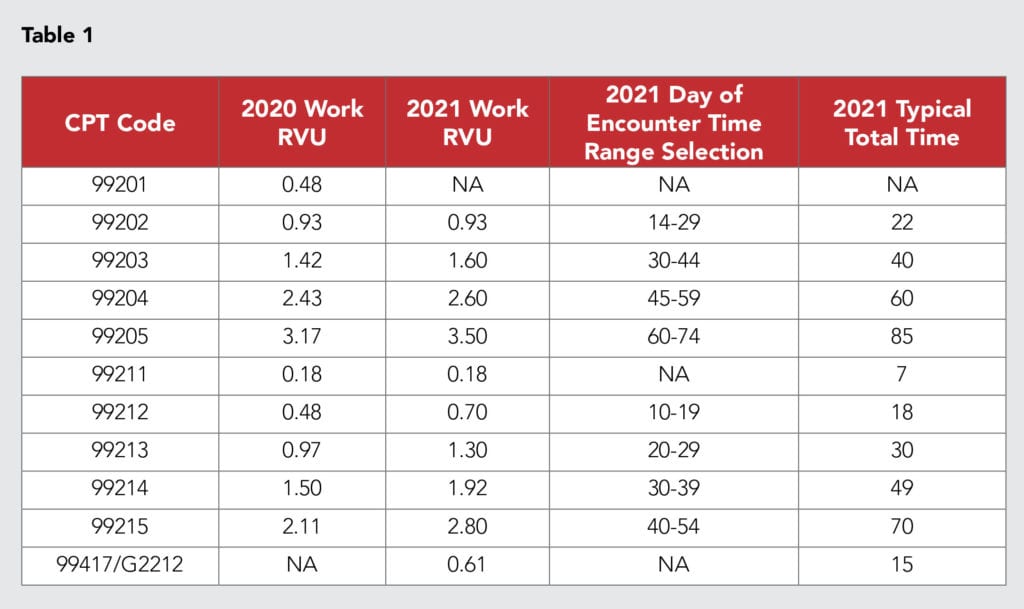
- Selection of the code level is based on either the newly defined level of medical decision making (MDM) or total time personally spent by the reporting practitioner on the day of the visit (includes face-to-face and non-face-to-face time) (see Table 1)
- The deletion of new patient code 99201 for 2021
- New prolonged services codes 99417 from CPT and G2212 from CMS for 15-minute increments beyond a level-5 service
Key 2021 CMS CPT Changes
Office/OP E&M codes:
- Codes 99202-99215 are now leveled based on MDM OR Total Time, no longer both.
- When time is the determining factor used to level the visit, that time is based on the total time of the visit (on the date of service) rather than on typical face-to-face time. Any record review prior to the actually seeing the patient, or post visit documentation of the visit must be performed on the date of the visit for the time to be included in the total time.
- HX and exam no longer scored-documentation to support medical necessity, however may still be needed to support medical necessity.
- New MDM grid is attached to assist physician in definitions, and required documentation and elements.
- Please note all other inpatient and other visit E&M codes leveling requirements remain the same (follow the 1995 & 1997 E/M guidelines).
- CMS has added two new Medicare specific G codes for reporting office/OP visit complexity.
- New separately reportable CPT codes for prolonged office/OP visits that are greater than 1 hr. Can only be billed with level 5 codes 99205 and 99211.
- New CPT codes for long-term continuous recorders, differentiated by 48hrs to 7 days and
- 7-15 days.
- New CPT codes for left heart arterial percutaneous VAD and left and right (venous) percutaneous VAD, as well as repositioning and removal of percutaneous left and right VAD.
- New Category III T codes for endovascular venous arterialization and substernal ICD implants.
- New Category III T code for pulmonary artery denervation.
Procedural Codes:
CMS increased the wRVU and reimbursement by 11% for codes 99202-99215, however in order to meet budget neutrality, they reduced the reimbursement and RVU for many of the cardiology procedural and imaging professional component.
Downloadable Resources
MedAxiom Coding Bootcamp – Evaluation & Management Pt. 1
MedAxiom Coding Bootcamp – Evaluation & Management Pt. 2
MedAxiom Coding Bootcamp – 2021 Coding Changes
CPT E/M Office Revisions – Level of Medical Decision Making (MDM)
Practice Management
A glance at 2021 evaluation and management changes
(HealthLeaders) – The evaluation and management (E/M) changes for calendar year 2021 are the result of a collaborative effort between the American Medical Association (AMA) and the Centers for Medicare & Medicaid Services (CMS).
CMS to audit some hospitals for price transparency compliance
(RevCycle Intelligence) – CMS is taking steps to ensure hospitals comply with a controversial price transparency rule taking effect on January 1, 2021.
AMA announces CPT codes for AstraZeneca’s COVID-19 vaccine
(Revenue Cycle Advisor) – The American Medical Association (AMA) recently updated the CPT code set to include immunization and administration codes for a COVID-19 vaccine under development by AstraZeneca and the University of Oxford.

Legislation & Rev Cylce
Analysis: 4 ways COVID-19 reshaped the revenue cycle
(RevCycle Intelligence) – In mid-March, COVID-19 reshaped almost everything about our world overnight, and the revenue cycle wasn’t spared. Entire departments were rapidly deployed to work from home, volumes plummeted, billing got pushed to the backburner, & the demand for digital tools ramped up.
Q&A: Preparing revenue cycle education for clinical staff
(Revenue Cycle Advisor) – Q: What are some key revenue cycle topics that should be included in education geared toward clinical staff?
New bill aims to ensure Medicare coverage for audio-only telehealth calls
(mHealth Intelligence) – A new bill before Congress aims to expand Medicare coverage for audio-only phone calls in telehealth programs. The Permanency for Audio-Only Telehealth Act, introduced last week by US Reps. Jason Smith (R-MO) and Tony Cardenas (D-CA), would have the Centers for Medicare & Medicaid Services reimburse care providers who use audio-only platforms for evaluation and management services as well as mental and behavioral health services. It would also remove CMS’ geographic restriction on the patient’s home as a delivery site for audio-only telehealth, and give the Health and Human Services Secretary that ability to add services for audio-only telehealth coverage.

Clinical & Quality
Cost-effectiveness favors anatomic over functional testing for stable chest pain
(TCTMD) – For the initial evaluation of low-risk patients with stable chest pain, anatomic testing—coronary CT angiography (CTA) with or without noninvasive fractional flow reserve (FFR)—is cost-effective compared with functional testing, a new analysis based on PROMISE trial data indicates.
CTO PCI techniques may be transferrable to peripheral vascular system
(ACC) – Techniques used in chronic total occlusion (CTO) PCI may be transferrable to the peripheral vascular system, according to a case published Dec. 16 in JACC: Case Reports.
After PCI for MI, 90-day prescriptions confer better medication adherence, fewer changes
(Healio) – Patients who filled out 90-day rather than 30-day prescriptions demonstrated higher adherence and infrequent medication changes following post-MI hospital discharge, researchers reported.
In Other News
Which conferences will still be virtual in 2021?
(Medscape) – When the COVID-19 pandemic exploded this past spring, medical conferences worldwide had to pivot quickly to online, virtual formats. Next year appears to be another year of transition, with the landscape of medical conference formats dotted with “virtual,” “in-person,” and “hybrid” meetings as the pandemic is expected to wane with the availability of effective vaccines.

Varied choices made by medical societies that have announced formats for next year reflect the struggle to safely bring large numbers of experts together nationally and internationally while preserving collegiality and an easy exchange of ideas.
Medscape’s review of nearly 70 conferences scheduled in 2021 finds that most meetings in the first quarter of the year will remain virtual. Beginning in March and April, more meetings are shifting either to a hybrid of in-person and virtual or in-person only.
However, organizers are also ready to change plans as the pandemic evolves, even for those conferences planned late in the year.
Mark G. Watson, MD, executive director for one of the largest conferences, the Radiological Society of North America (RSNA), told Medscape Medical News that, for now, its conference is scheduled to be an in-person meeting in Chicago in December 2021, with a planned virtual component as well.
“However,” he said, “RSNA will continue to monitor the global situation and will be ready to provide a high-quality experience for our attendees and exhibitors, whatever the forum.”
Philip Masters, MD, vice president of membership for the American College of Physicians (ACP), told Medscape Medical News that pandemic uncertainty pushed ACP to go virtual for its late-April 2021 meeting. The conference typically draws between 10,000 and 15,000 people.
“There’s a huge amount of uncertainty about the trajectory of the pandemic even if we do have a vaccine,” he said. “Bringing that many medical professionals into one place where they could infect each other or bring [the virus] back to their patients is not a good idea.”
Moving large numbers of people from room to room with social distancing also presents huge space and time challenges, he noted. In addition, some major academic institutions have asked faculty not to travel. Even where travel is permitted, some medical professionals may simply feel unsafe traveling.
Some large meetings haven’t committed either way. The American Medical Association website for its 2021 House of Delegates meeting, for instance, says, “More details to follow. Dates and locations subject to change.”